HOME | ABOUT US | MEDIA KIT | CONTACT US | INQUIRE
HOME | ABOUT US | MEDIA KIT | CONTACT US | INQUIRE

Let’s face it: As a region, with the medical resources available to us, we are truly blessed.
How so? Just this spring, the Kaiser Family Foundation ranked states by the number of hospital beds available per 1,000 residents. Kansas tied for seventh place at 3.3; Missouri was tied for No. 13 at 3.1.
“Fine,” you say. “So what?” The thing is, a bed by itself does no hospital or health system any good unless it has medical professionals in place to attend patient needs. More beds equals more providers. And in a market as competitive as Kansas City’s, in an era where a doctor’s every move is subject to an on-line patient-review platform, it all adds up to more top-tier talent to provide that care.
 Nowhere does that elevated level of care present itself for inspection quite the way it does with Ingram’s annual Top Doctors awards. We launched this recognition program in 1997, with one key criterion for consideration: If you or a close family member were the patient, which physician would you turn to? That’s not an invitation to nominate co-workers, pals or your brother-in-law. At that level, it’s personal.
Nowhere does that elevated level of care present itself for inspection quite the way it does with Ingram’s annual Top Doctors awards. We launched this recognition program in 1997, with one key criterion for consideration: If you or a close family member were the patient, which physician would you turn to? That’s not an invitation to nominate co-workers, pals or your brother-in-law. At that level, it’s personal.
That’s why we put so much stock in the advice, guidance and counsel we get from past honorees each year. They know good care, and they know where they would go to get it if their own health depended on it.
The interesting thing about the changing face of quality care in this region is how we’re able to attract talent from, quite literally, all over the world. This year’s class of 14 Top Doctors includes some who hail from Greece, Jordan, India and Sri Lanka. And a fair number who grew up here, studied medicine here, trained here and set down their roots to deliver that quality of compassionate care in their hometowns.
Not surprisingly, the scales favoring inclusion with this year’s class tipped just a bit in favor of physicians who are on the front lines battling the biggest health crisis in a century. Top Doctors has always been defined by physicians who go above and beyond to deliver care, but this past year has created opportunities—no, it’s more like demands—for a higher level of commitment from workers across the health-care spectrum.
For their outstanding levels of care, for the tireless efforts in the face of a global killer, for their career-long dedication and commitment, we proudly recognize the 14 newest members of Ingram’s Top Doctors. Please join us in saluting their achievements, and their contributions. What they do makes this a great place to be alive … and to stay that way.
 Sometimes, Eyad Al-hihi can tell you, it’s the unexpected moment with a patient that can validate a career’s worth of work. You can see it in his description of a diabetic patient he once treated, a man with a foot infection that had developed gangrene. “We made to make a decision to amputate his foot,” Al-hihi recalls. “I discussed with him and he was very upset and did not want to do that, so I told him that he will need to make this decision so we can save his life.” The patient finally relented and during the course of his recovery, they met again. This time, there was no sign of distress. “I asked him how he feels,” Al-hihi said. “He smiled and said that he is blessed. I was surprised and I asked him why. He said that he is blessed that he is alive and that he has another foot. That affected me and made me always think and look at things in different lenses.” That’s just one example of the life-affirming experiences Al-hihi has gleaned over the course of 25 years since earning his medical degree in his native Jordan. “I wanted to be part of removing sufferings and curing sick people,” he says of his motivation to become a doctor. “When I was a child, I lost some family members to illnesses and I was fascinated by medicine as a career to cure and treat others.” He carried that interest into primary care, a model he says is based on trust and building relationships. “I find it rewarding to work with my patients on chronic disease management and prevention. I also enjoy my practice as a hospitalist, taking care of acutely ill patients and using my knowledge and skills and remove their pain and suffering.” The values he brings to those relationships were formed in his youth, he says. “I was raised by my family to recognize all the blessings I have and to be grateful. My parents were teachers and I realized that learning is a life long journey, and not a destination. I have several values that shaped my career including respect to all, patience, persistence, and team dynamics.” After stints in Canada and in Michigan and Pennsylvania to complete his training, he decided Kansas City would be his destination. His training may be a quarter-century behind him, but he’s still learning about the power of medicine to cure. Never has that been more evident than during the past eight months in the age of COVID-19. “The COVID19 pandemic taught me that we should always plan ahead and not take things for granted,” Al-hihi says. “We need to invest more in pandemic preparedness and public health. We also need to count our blessings and value our ability to socialize with each other. The pandemic also taught us to be creative in the way we live, teach, learn, interact, and work.”
Sometimes, Eyad Al-hihi can tell you, it’s the unexpected moment with a patient that can validate a career’s worth of work. You can see it in his description of a diabetic patient he once treated, a man with a foot infection that had developed gangrene. “We made to make a decision to amputate his foot,” Al-hihi recalls. “I discussed with him and he was very upset and did not want to do that, so I told him that he will need to make this decision so we can save his life.” The patient finally relented and during the course of his recovery, they met again. This time, there was no sign of distress. “I asked him how he feels,” Al-hihi said. “He smiled and said that he is blessed. I was surprised and I asked him why. He said that he is blessed that he is alive and that he has another foot. That affected me and made me always think and look at things in different lenses.” That’s just one example of the life-affirming experiences Al-hihi has gleaned over the course of 25 years since earning his medical degree in his native Jordan. “I wanted to be part of removing sufferings and curing sick people,” he says of his motivation to become a doctor. “When I was a child, I lost some family members to illnesses and I was fascinated by medicine as a career to cure and treat others.” He carried that interest into primary care, a model he says is based on trust and building relationships. “I find it rewarding to work with my patients on chronic disease management and prevention. I also enjoy my practice as a hospitalist, taking care of acutely ill patients and using my knowledge and skills and remove their pain and suffering.” The values he brings to those relationships were formed in his youth, he says. “I was raised by my family to recognize all the blessings I have and to be grateful. My parents were teachers and I realized that learning is a life long journey, and not a destination. I have several values that shaped my career including respect to all, patience, persistence, and team dynamics.” After stints in Canada and in Michigan and Pennsylvania to complete his training, he decided Kansas City would be his destination. His training may be a quarter-century behind him, but he’s still learning about the power of medicine to cure. Never has that been more evident than during the past eight months in the age of COVID-19. “The COVID19 pandemic taught me that we should always plan ahead and not take things for granted,” Al-hihi says. “We need to invest more in pandemic preparedness and public health. We also need to count our blessings and value our ability to socialize with each other. The pandemic also taught us to be creative in the way we live, teach, learn, interact, and work.”
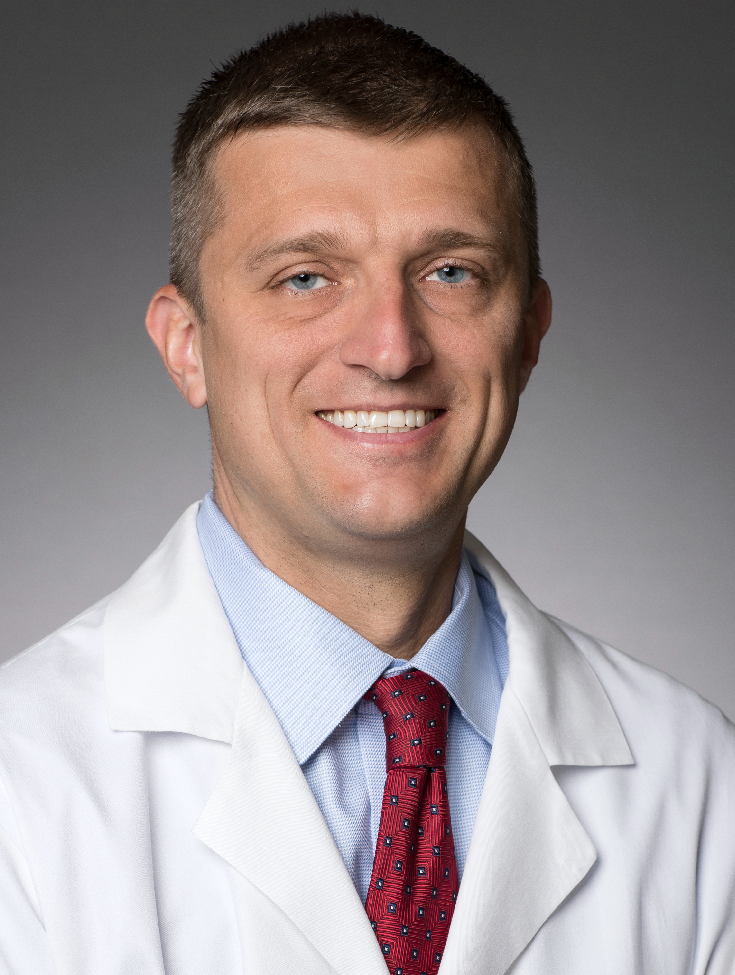 Nearly 15 years later, the moment lives on with David Anderson—especially when he’s faced with a complex orthopedic challenge. Before his graduation from Creighton University’s School of Medicine, he recalls, chaplain Marcia Cusic “took me aside and gave a blessing to my hands, reminding me that the ability to do surgery is a gift and that she had high hopes for me to help other people. I think about that often.” A Kansas City native and Rockhurst High grad, he learned about mechanics early in life: First, the operation of a human body in wrestling, track and cross-country, and then the engineering and machining instruction at his father’s auto machine shop. “Most of the skills I have with my hands were refined learning how to machine and build engines for
Nearly 15 years later, the moment lives on with David Anderson—especially when he’s faced with a complex orthopedic challenge. Before his graduation from Creighton University’s School of Medicine, he recalls, chaplain Marcia Cusic “took me aside and gave a blessing to my hands, reminding me that the ability to do surgery is a gift and that she had high hopes for me to help other people. I think about that often.” A Kansas City native and Rockhurst High grad, he learned about mechanics early in life: First, the operation of a human body in wrestling, track and cross-country, and then the engineering and machining instruction at his father’s auto machine shop. “Most of the skills I have with my hands were refined learning how to machine and build engines for
antique autos and race cars, which are passions I still try to enjoy in my time off,” says Anderson, whose practice, Kansas City Joint Replacement and Sports Medicine, is part of HCA Midwest Health. His first exposure to medicine involved stories of patients with four legs, recounted by his grandfather, a retired veterinarian, as young David marveled at his surgical tools. That would have been his path, too, but for exposure to human anatomy in high school and a chance connection with an orthopedic surgeon who mended his Dad’s fractured ankle. “After shadowing him in the operating room and in his clinic, I realized that this was something I could do and enjoy my entire career,” Anderson said. What’s the particular allure of orthopedic surgery? “For me, it’s the mechanical nature and three-dimensional thinking it takes to reliably repair a diseased hip or knee joint,” he says. “In my interviews for residency, my answer was always that “ ‘I really like to fix things.’” Digital technology, he says, allows those in his craft to produce patient-specific solutions that improve on already-established treatment regimens. On top of that, he says, “I have been fortunate in my career to be able to work with excellent orthopedic mentors and colleagues who are thought leaders in the field to hopefully improve the high quality care that we have available in Kansas City.” Like all orthopedic specialists, he wrestles with the challenges of the pandemic and its effect on in-person treatments. “For a surgeon who relies on physical exam, as much as I rely on imaging, it is tough to treat what we do completely on a telemedicine or digital alternative,” he says. Patients in general, he says, just want assurances that hospitals and doctors “are being ethical and thoughtful in how we provide care so they are safe getting through any visit or procedure.”
 Here’s the thing about internal medicine: You problem-solve for a whole lot of medical specialties downstream, so it starts with your detective work. And for Larry Botts, there’s been a lot of that work to do the past eight months, since a little bug from Wuhan jumped containment and turned into a global nightmare. But here’s another thing about internists: They are quick studies. And Botts, who doubles as chief medical officer for the medical center in Merriam, will tell you up front: “We are infinitely better at treating this disease than we were in March and April. Treatment continued to improve, and I suspect it will even more. But this will be with us for a while, no doubt.” The impact on health-care workers has been pronounced; more than 200,000 have died nationwide from it. For those who have been able to recover from it, or stave it off while working extra hours, “there is the problem of burnout,” Botts says. “That’s not something new; we talked about it before COVID was here. But in recent years, it’s been more of a concern because we’ve lost a lot of good physicians and nurses. The reasons are complex, a solution is not quick to come, but this has created a greater urgency to look at ways to take care of those taking care of patients.” Born and raised in Omaha, Botts learned a bit about caregiving early, as the oldest of five siblings. “I got a head start on responsibility and leadership at home,” he says, where he was fortunate enough to have parents who stressed the importance of education. His schooling veered toward engineering, but he found himself drawn to life sciences and changed majors to biology, then physiology. Working as an EKG tech, he said, he discovered that “what I wanted to do was use my love of life sciences to take care of people, instead of doing research.” Patient interactions on his medical school rotations proved to be most rewarding, and their cases presented that intellectual challenge, especially with the critically ill in intensive care. “It was mostly the challenge, but there was a lot of satisfaction, when they would eventually leave ICU and fully recover,” Botts says. Being an internist means accepting the sheer numbers of decisions that must be made, and the speed required, before referring patients to surgeons or other specialists. “Solving that riddle of what’s wrong—that’s being a critical-care physician, seeing a wide variety of patients in an intensive-care setting, then having to decide which direction you have to go,” he says. That’s an additional layer of stress, “but fortunately, I had the kind of demeanor that was conducive to ICU.”
Here’s the thing about internal medicine: You problem-solve for a whole lot of medical specialties downstream, so it starts with your detective work. And for Larry Botts, there’s been a lot of that work to do the past eight months, since a little bug from Wuhan jumped containment and turned into a global nightmare. But here’s another thing about internists: They are quick studies. And Botts, who doubles as chief medical officer for the medical center in Merriam, will tell you up front: “We are infinitely better at treating this disease than we were in March and April. Treatment continued to improve, and I suspect it will even more. But this will be with us for a while, no doubt.” The impact on health-care workers has been pronounced; more than 200,000 have died nationwide from it. For those who have been able to recover from it, or stave it off while working extra hours, “there is the problem of burnout,” Botts says. “That’s not something new; we talked about it before COVID was here. But in recent years, it’s been more of a concern because we’ve lost a lot of good physicians and nurses. The reasons are complex, a solution is not quick to come, but this has created a greater urgency to look at ways to take care of those taking care of patients.” Born and raised in Omaha, Botts learned a bit about caregiving early, as the oldest of five siblings. “I got a head start on responsibility and leadership at home,” he says, where he was fortunate enough to have parents who stressed the importance of education. His schooling veered toward engineering, but he found himself drawn to life sciences and changed majors to biology, then physiology. Working as an EKG tech, he said, he discovered that “what I wanted to do was use my love of life sciences to take care of people, instead of doing research.” Patient interactions on his medical school rotations proved to be most rewarding, and their cases presented that intellectual challenge, especially with the critically ill in intensive care. “It was mostly the challenge, but there was a lot of satisfaction, when they would eventually leave ICU and fully recover,” Botts says. Being an internist means accepting the sheer numbers of decisions that must be made, and the speed required, before referring patients to surgeons or other specialists. “Solving that riddle of what’s wrong—that’s being a critical-care physician, seeing a wide variety of patients in an intensive-care setting, then having to decide which direction you have to go,” he says. That’s an additional layer of stress, “but fortunately, I had the kind of demeanor that was conducive to ICU.”
 Childhood memories of a favorite aunt would help form a deeply personal motivation for Karla Houston-Gray’s decision to become a doctor. “My aunt, who I was very close to when I was a small child, passed away while living in a rural part of Florida,” Houston-Gray says. “I remember hoping she could get to the doctor, but access to health care was very tough, especially in a rural areas. I felt if the medical care in that rural area would have been better, she may have had a better chance of surviving.” It was her passion for people and the sciences, she said, that drove her to pursue a career in medicine. That led her to New Orleans, where she earned her medical degree from the Tulane University, followed by residency at the University of Kansas Medical Center in Kansas City, Kan., where she focused on internal medicine and continues to specialize in treatment of hypertension and diabetes. “Internal medicine,” Houston-Gray says, “encompasses a lot of medical specialties” and it represents health care’s first line of defense for patients, treating “everything from high blood pressure, high cholesterol, diabetes, shots and immunizations—you name it, we deal with it.” Her approach to patient care, she says, is informed by values she developed in her youth, thanks in part to what she called “a hard-working family.” That started with her grandfather, who “inspired me to think big and pursue my dreams,” she says. “As a child I used to play doctor practicing on both of my grandparents.” She finds both personal and professional rewards in serving a patient population near Kansas City’s urban core. “I feel they need excellent health care just as much as a people in other areas do,” she says. “It’s nice when you treat patients, then their kids, then their kids. It brings me great joy in treating the family. I love my patients. I love caring for people.” She’s able to engage with patients from her base at Midwest Metropolitan Physicians Group and Research Medical Center, the market flagship for HCA Midwest Health. And through those interactions, she reaches career-affirming outcomes. “I have experiences every day that speak to me that this is why I do what I do,” Houston-Gray says. “I see people I’ve encouraged who decide to quit smoking after years; see people make health and fitness decisions that decrease their cholesterol or their blood sugar level. This is why I love being a doctor.”
Childhood memories of a favorite aunt would help form a deeply personal motivation for Karla Houston-Gray’s decision to become a doctor. “My aunt, who I was very close to when I was a small child, passed away while living in a rural part of Florida,” Houston-Gray says. “I remember hoping she could get to the doctor, but access to health care was very tough, especially in a rural areas. I felt if the medical care in that rural area would have been better, she may have had a better chance of surviving.” It was her passion for people and the sciences, she said, that drove her to pursue a career in medicine. That led her to New Orleans, where she earned her medical degree from the Tulane University, followed by residency at the University of Kansas Medical Center in Kansas City, Kan., where she focused on internal medicine and continues to specialize in treatment of hypertension and diabetes. “Internal medicine,” Houston-Gray says, “encompasses a lot of medical specialties” and it represents health care’s first line of defense for patients, treating “everything from high blood pressure, high cholesterol, diabetes, shots and immunizations—you name it, we deal with it.” Her approach to patient care, she says, is informed by values she developed in her youth, thanks in part to what she called “a hard-working family.” That started with her grandfather, who “inspired me to think big and pursue my dreams,” she says. “As a child I used to play doctor practicing on both of my grandparents.” She finds both personal and professional rewards in serving a patient population near Kansas City’s urban core. “I feel they need excellent health care just as much as a people in other areas do,” she says. “It’s nice when you treat patients, then their kids, then their kids. It brings me great joy in treating the family. I love my patients. I love caring for people.” She’s able to engage with patients from her base at Midwest Metropolitan Physicians Group and Research Medical Center, the market flagship for HCA Midwest Health. And through those interactions, she reaches career-affirming outcomes. “I have experiences every day that speak to me that this is why I do what I do,” Houston-Gray says. “I see people I’ve encouraged who decide to quit smoking after years; see people make health and fitness decisions that decrease their cholesterol or their blood sugar level. This is why I love being a doctor.”
 At 11,000 residents, Camden, Ark., isn’t as big today as it was when Bridgette Jones was growing up there—The Gateway to Smackover had a population of 15,000-plus in those days—but the folks living there proved to be mighty influential. Her parents of course, a schoolteacher and a worker at the International Paper factory, but also grandparents on both sides who provided this only child with vital support and nurturing. They instilled in her a sense of self-confidence, not arrogance. She could grow up to be anything she wanted to be—and did. Jones carries that same sense of nurturing with her today as an asthma-allergy specialist at Children’s Mercy Hospital. “I remember wanting to be a doctor since a very early age,” she says, and proof of that hangs in her office today: A picture she drew in first grade, depicting herself as a doctor at a patient’s bedside. Perhaps some of the influence came from trips to the doctor with her maternal grandmother, who had diabetes and hypertension. “She passed away when I was 14. It put something inside me that I wanted to provide care for people like my grandmother and other family members.” A lifelong love for being around children led her to pediatrics, and her medical school rotations, she says, confirmed it was the right choice. “Immunology was not so much in the plan or my head, but I realized that I was drawn to the patients that had asthma the most,” she said. Small tweaks in care protocols could produce significant outcomes and let children live more like children should. “When you see a child with breathing difficulties not able to play their favorite sport, run at recess without getting out of breath, then start them on meds, and eventually be able to play sports or run like any other child—I found it extremely rewarding to see those differences you could make.” She harkens back to the lessons of her youth in raising her two young girls. “I’m pretty sure we didn’t have any female doctors that I can remember, and we certainly didn’t have black physicians until I was in middle school—my cousin was first black doctor,” she say, so it’s important for them to see a variety of positions they can relate to. That view ties in with her additional role as the hospital’s director of diversity and equity, “another important aspect of what we do to provide quality in care for all patients,” Jones says. “Again, it was not something I planned to do, it just happened organically, seeing the need for diverse voices at the table in medical care and institutions. To meet the needs of all patients that walk in our doors, diversity is key. You can see it in pretty much everything now.”
At 11,000 residents, Camden, Ark., isn’t as big today as it was when Bridgette Jones was growing up there—The Gateway to Smackover had a population of 15,000-plus in those days—but the folks living there proved to be mighty influential. Her parents of course, a schoolteacher and a worker at the International Paper factory, but also grandparents on both sides who provided this only child with vital support and nurturing. They instilled in her a sense of self-confidence, not arrogance. She could grow up to be anything she wanted to be—and did. Jones carries that same sense of nurturing with her today as an asthma-allergy specialist at Children’s Mercy Hospital. “I remember wanting to be a doctor since a very early age,” she says, and proof of that hangs in her office today: A picture she drew in first grade, depicting herself as a doctor at a patient’s bedside. Perhaps some of the influence came from trips to the doctor with her maternal grandmother, who had diabetes and hypertension. “She passed away when I was 14. It put something inside me that I wanted to provide care for people like my grandmother and other family members.” A lifelong love for being around children led her to pediatrics, and her medical school rotations, she says, confirmed it was the right choice. “Immunology was not so much in the plan or my head, but I realized that I was drawn to the patients that had asthma the most,” she said. Small tweaks in care protocols could produce significant outcomes and let children live more like children should. “When you see a child with breathing difficulties not able to play their favorite sport, run at recess without getting out of breath, then start them on meds, and eventually be able to play sports or run like any other child—I found it extremely rewarding to see those differences you could make.” She harkens back to the lessons of her youth in raising her two young girls. “I’m pretty sure we didn’t have any female doctors that I can remember, and we certainly didn’t have black physicians until I was in middle school—my cousin was first black doctor,” she say, so it’s important for them to see a variety of positions they can relate to. That view ties in with her additional role as the hospital’s director of diversity and equity, “another important aspect of what we do to provide quality in care for all patients,” Jones says. “Again, it was not something I planned to do, it just happened organically, seeing the need for diverse voices at the table in medical care and institutions. To meet the needs of all patients that walk in our doors, diversity is key. You can see it in pretty much everything now.”
 A career in medicine? Didn’t seem like it would be in the cards for Clif Jones. “I remember from an early age being uncomfortable around people with illness,” he remembers. Which wasn’t a problem back then; coming from a K-State faculty family in Manhattan, it seemed he’d be destined for academia, in any case. Even though it took a while, he found his path. First came the college biology track, then a move to microbiology, thanks to the influence of a bacteriologist/biochemist faculty member. And before long, he was applying for medical school, for reasons that still escape him today. “Friends in pre-medicine or medical school at the time wondered how I ever got accepted without being able to explain to interviewers why I wanted to be a physician,” says Jones, now an infectious-disease specialist for Stormont Vail Health in Topeka. “I truly did not know why at that time.” What he learned from peers, mentors and patients, he says, was “that I could be competent providing care, and was directed to internal medicine and then to infectious diseases as a clinical practice.” Diagnosis and treatment of infectious diseases stand at the intersection of internal medicine and his longstanding interest in microbiology, Jones says. “If hospital-based internal medicine would have been a career option 30 years ago, I might not have pursued fellowship training in infectious diseases,” he confesses. “But I’ve never regretted that decision and I love being a consultant in this field.” Today, he’s part of the regional fight against one of the great infectious-disease challenges of the past century. “The COVID-19 pandemic has changed so many facets in the delivery of health care, to the point where we’re finding great joy in traditional clinical encounters, whether in the clinic or the hospital,” Jones says. Hallway consultations, always a pleasure, require literally milling around in the corridors either on nursing units or between them, he says, but are now a great rarity, given the need to maintain safe distance. “When I actually see one of the surgeons or hospitalists in person, for just that instant, it feels like old times,” he says. Over the course of 30 years in medicine, he can recall instances in which stubborn clinical problems yielded to a combination of competency and luck, with positive patient outcomes. But that coin has a flip side, where despite your best efforts, you can’t save a patient. Given that, he says, “it’s best sometimes not to just focus on the spectacular.”
A career in medicine? Didn’t seem like it would be in the cards for Clif Jones. “I remember from an early age being uncomfortable around people with illness,” he remembers. Which wasn’t a problem back then; coming from a K-State faculty family in Manhattan, it seemed he’d be destined for academia, in any case. Even though it took a while, he found his path. First came the college biology track, then a move to microbiology, thanks to the influence of a bacteriologist/biochemist faculty member. And before long, he was applying for medical school, for reasons that still escape him today. “Friends in pre-medicine or medical school at the time wondered how I ever got accepted without being able to explain to interviewers why I wanted to be a physician,” says Jones, now an infectious-disease specialist for Stormont Vail Health in Topeka. “I truly did not know why at that time.” What he learned from peers, mentors and patients, he says, was “that I could be competent providing care, and was directed to internal medicine and then to infectious diseases as a clinical practice.” Diagnosis and treatment of infectious diseases stand at the intersection of internal medicine and his longstanding interest in microbiology, Jones says. “If hospital-based internal medicine would have been a career option 30 years ago, I might not have pursued fellowship training in infectious diseases,” he confesses. “But I’ve never regretted that decision and I love being a consultant in this field.” Today, he’s part of the regional fight against one of the great infectious-disease challenges of the past century. “The COVID-19 pandemic has changed so many facets in the delivery of health care, to the point where we’re finding great joy in traditional clinical encounters, whether in the clinic or the hospital,” Jones says. Hallway consultations, always a pleasure, require literally milling around in the corridors either on nursing units or between them, he says, but are now a great rarity, given the need to maintain safe distance. “When I actually see one of the surgeons or hospitalists in person, for just that instant, it feels like old times,” he says. Over the course of 30 years in medicine, he can recall instances in which stubborn clinical problems yielded to a combination of competency and luck, with positive patient outcomes. But that coin has a flip side, where despite your best efforts, you can’t save a patient. Given that, he says, “it’s best sometimes not to just focus on the spectacular.”
 The operating room surgeon or ER physician is usually the one depicted on most of those network TV dramas; ditto for the officer nabbing the bad guy in the police melodramas. Maybe it’s time to wed the best of medicine and investigative work and give Kamani Lankachandra her own show: After all, she combines the laboratory challenge of solving medical riddles with her mission to help diagnose patients suffering from all sorts of maladies. She’s been a pathologist at Truman Medical Centers since 1996, following a series of globe-trotting that took her from her native Sri Lanka, where she earned her medical degree, to the United Kingdom, then stateside with her first post at the University of Maryland for training in her specialty. At that point, she came to Truman, and also accepted a teaching position at UMKC’s school of medicine. “I always wanted to do medicine; I don’t remember a particular reason behind it,” Lankachandra says. But pathology was a different story. “I loved pathology during my medical school, she says. “My friends thought that was weird; not many medical students would have an aspiration to be a pathologist, to tell the truth. I like the critical nature and problem-solving aspect of pathology.” Especially at Truman, she says, which “gives me the resources and the freedom to do what I do. I am eternally grateful.” While the bulk of her work is in the lab, her connections with patients have produced some lasting memories. One of those involved a man who came to her office, concerned about a large lump in his neck. “I performed a procedure (fine needle aspiration) and found out it was cancer,” she said. “We had a long conversation and he started crying. I somehow managed to get TMC financial counselling to help him and got him in for treatment. I thought about TMC physicians who encounter similar patients every day, this is why we do what we do at Truman.” Of course, what they do at Truman has changed this year, thanks to COVID-19. Its impact on hospital operations has been profound, but was especially so in the late winter as the outbreak started. “This pandemic changed all of our lives, the way we do everything,” Lankachandra says. “The first two weeks were daunting; I didn’t know how to respond to anything. “Soon we regrouped—our TMC lab team became one big family,” she says. “We all came to work without missing a day, and work we did! TMC administration was amazing, even to this date. They provided us with guidance, support and resources to do the job. TMC Incident Command Center became our life line for information and resources.”
The operating room surgeon or ER physician is usually the one depicted on most of those network TV dramas; ditto for the officer nabbing the bad guy in the police melodramas. Maybe it’s time to wed the best of medicine and investigative work and give Kamani Lankachandra her own show: After all, she combines the laboratory challenge of solving medical riddles with her mission to help diagnose patients suffering from all sorts of maladies. She’s been a pathologist at Truman Medical Centers since 1996, following a series of globe-trotting that took her from her native Sri Lanka, where she earned her medical degree, to the United Kingdom, then stateside with her first post at the University of Maryland for training in her specialty. At that point, she came to Truman, and also accepted a teaching position at UMKC’s school of medicine. “I always wanted to do medicine; I don’t remember a particular reason behind it,” Lankachandra says. But pathology was a different story. “I loved pathology during my medical school, she says. “My friends thought that was weird; not many medical students would have an aspiration to be a pathologist, to tell the truth. I like the critical nature and problem-solving aspect of pathology.” Especially at Truman, she says, which “gives me the resources and the freedom to do what I do. I am eternally grateful.” While the bulk of her work is in the lab, her connections with patients have produced some lasting memories. One of those involved a man who came to her office, concerned about a large lump in his neck. “I performed a procedure (fine needle aspiration) and found out it was cancer,” she said. “We had a long conversation and he started crying. I somehow managed to get TMC financial counselling to help him and got him in for treatment. I thought about TMC physicians who encounter similar patients every day, this is why we do what we do at Truman.” Of course, what they do at Truman has changed this year, thanks to COVID-19. Its impact on hospital operations has been profound, but was especially so in the late winter as the outbreak started. “This pandemic changed all of our lives, the way we do everything,” Lankachandra says. “The first two weeks were daunting; I didn’t know how to respond to anything. “Soon we regrouped—our TMC lab team became one big family,” she says. “We all came to work without missing a day, and work we did! TMC administration was amazing, even to this date. They provided us with guidance, support and resources to do the job. TMC Incident Command Center became our life line for information and resources.”
 The last image of Greece that 11-year-old Demetrios Maragos saw as his family’s journey to America began was at the Acropolis, high on the hill over Athens. “Fast-forward 18 hours, and we’re in Omaha, and I’m looking at a corn field from my hotel room!” he marvels. His father, a pediatrician, had uprooted the family to teach at Creighton University, and young Demetrios would begin his American experience with a series of 78-rpm Berlitz English instructional records. So, no, it wasn’t the smoothest transition any preteen had ever gone through, “but giving up the only home I’d ever known as possibly one of the greatest things that ever happened to me, in hindsight,” he says, but it would also pay off for thousands of cardiology patients over the next 30 years. In college back east, he flirted with architectural studies. “But I would go to watch my father in his office, interacting with patients, and saw the love and tenderness with them, and it just impressed me,” he says. Neither he nor his brother, he says, were prodded to go into medicine, but both ended up becoming physicians. In his case, it came after a number of open courses in college prompted him to take the MCAT: “Once I decided that, it was easy” to go into medicine, he says. Cardiology revealed its particular appeal during his rotations. “I loved the discrete nature of it, the heart, and how it works as an organ, how important it is.” Combined with good mentors, Maragos says, everything just clicked. A fellowship at Saint Luke’s Mid-America Heart Institute introduced him to Kansas City, and he found here the same kinds of values he came to know in Omaha. Kansas City it would be. Like the rest of the staff at Liberty Hospital, and medical professionals everywhere, he’s still wrestling with the effects of a global pandemic—an infectious disease that has left a footprint on every phase of health-care delivery. “It was such a rapid transition,” Maragos says, “back in mid-March when everything pretty much shut down, how quickly hospitals, offices and clinics had to transition the way we provide care to preserve the safety of patients and staff.” After 27 years, he’s starting to see patients who are the children of earlier cases he’d managed long ago, and he finds comfort in those relationships. “After 26 years, you see someone come and I ask, ‘Do I know you?’ and they say ‘you took care of my grandfather 20 years ago.’ To me, that is one of the most heartwarming things—people want to come back and see you because of a connection you made long ago, under strenuous circumstances.”
The last image of Greece that 11-year-old Demetrios Maragos saw as his family’s journey to America began was at the Acropolis, high on the hill over Athens. “Fast-forward 18 hours, and we’re in Omaha, and I’m looking at a corn field from my hotel room!” he marvels. His father, a pediatrician, had uprooted the family to teach at Creighton University, and young Demetrios would begin his American experience with a series of 78-rpm Berlitz English instructional records. So, no, it wasn’t the smoothest transition any preteen had ever gone through, “but giving up the only home I’d ever known as possibly one of the greatest things that ever happened to me, in hindsight,” he says, but it would also pay off for thousands of cardiology patients over the next 30 years. In college back east, he flirted with architectural studies. “But I would go to watch my father in his office, interacting with patients, and saw the love and tenderness with them, and it just impressed me,” he says. Neither he nor his brother, he says, were prodded to go into medicine, but both ended up becoming physicians. In his case, it came after a number of open courses in college prompted him to take the MCAT: “Once I decided that, it was easy” to go into medicine, he says. Cardiology revealed its particular appeal during his rotations. “I loved the discrete nature of it, the heart, and how it works as an organ, how important it is.” Combined with good mentors, Maragos says, everything just clicked. A fellowship at Saint Luke’s Mid-America Heart Institute introduced him to Kansas City, and he found here the same kinds of values he came to know in Omaha. Kansas City it would be. Like the rest of the staff at Liberty Hospital, and medical professionals everywhere, he’s still wrestling with the effects of a global pandemic—an infectious disease that has left a footprint on every phase of health-care delivery. “It was such a rapid transition,” Maragos says, “back in mid-March when everything pretty much shut down, how quickly hospitals, offices and clinics had to transition the way we provide care to preserve the safety of patients and staff.” After 27 years, he’s starting to see patients who are the children of earlier cases he’d managed long ago, and he finds comfort in those relationships. “After 26 years, you see someone come and I ask, ‘Do I know you?’ and they say ‘you took care of my grandfather 20 years ago.’ To me, that is one of the most heartwarming things—people want to come back and see you because of a connection you made long ago, under strenuous circumstances.”
 Lifelong learning, service to others, and respect for all people. Those aren’t necessarily the focus of a medical school education, but they are foundational elements of superior care for anyone who aspires to be a physician. And they were front-loaded into Alexis Meredith growing up in Kansas City, Kan. This Sumner Academy of Arts and Science graduate, while working toward a biology degree at K-State, says she “chose that as a major without knowing where that would lead.” But a chance opportunity to shadow a local physician in clinic yielded her a-ha! moment. “I was struck by the vast knowledge that she had, in addition to the connections that she had developed with her patients,” she recalls. “The trust that they placed in her made it clear that medicine was the right field for me.” At KU’s school of medicine, she found her calling during a fourth-year rotation in ICU. “I learned from wonderful mentors in the field both as an internal medicine resident and then as a pulmonary/critical care fellow at KU.” Those disciplines, she says, required the ability to take a large amount of information and condense that into a diagnosis and treatment plan for each patient. “More than that, it allowed me to become an advocate and counselor for my patients and their families at some of life’s most difficult moments. … I also saw how taking the time to listen and know them personally helped them feel less scared and more in control of their situation. I have learned that being able to help patients and their families during their most stressful moments is the true privilege of being a doctor.” The deep relationships she can forge with patients are especially meaningful; they are what she relishes about pulmonary and critical-care medicine. “I had a very special patient that I cared for throughout her battle with pulmonary fibrosis,” Meredith remembers. “She and her husband adopted a cat and chose to name it after me. The patient has since passed on, but the cat lives on. It sits on her husband’s CPAP machine and turns it off for him every morning. The fact that a part of my bond with her lives on makes me exceedingly happy.” Communication has always been at the heart of such relationships, and never has it been more important in remaining connected with patients than in 2020. “The recent pandemic has created new challenges for everyone, including the health-care system,” Meredith says. “For me, it has reinforced the critical importance of communication in health care. The pandemic has impacted the way that we care for patients directly, the way that we keep their families involved and updated while their loved one is hospitalized, and the way that we communicate with community leaders and with other physicians.”
Lifelong learning, service to others, and respect for all people. Those aren’t necessarily the focus of a medical school education, but they are foundational elements of superior care for anyone who aspires to be a physician. And they were front-loaded into Alexis Meredith growing up in Kansas City, Kan. This Sumner Academy of Arts and Science graduate, while working toward a biology degree at K-State, says she “chose that as a major without knowing where that would lead.” But a chance opportunity to shadow a local physician in clinic yielded her a-ha! moment. “I was struck by the vast knowledge that she had, in addition to the connections that she had developed with her patients,” she recalls. “The trust that they placed in her made it clear that medicine was the right field for me.” At KU’s school of medicine, she found her calling during a fourth-year rotation in ICU. “I learned from wonderful mentors in the field both as an internal medicine resident and then as a pulmonary/critical care fellow at KU.” Those disciplines, she says, required the ability to take a large amount of information and condense that into a diagnosis and treatment plan for each patient. “More than that, it allowed me to become an advocate and counselor for my patients and their families at some of life’s most difficult moments. … I also saw how taking the time to listen and know them personally helped them feel less scared and more in control of their situation. I have learned that being able to help patients and their families during their most stressful moments is the true privilege of being a doctor.” The deep relationships she can forge with patients are especially meaningful; they are what she relishes about pulmonary and critical-care medicine. “I had a very special patient that I cared for throughout her battle with pulmonary fibrosis,” Meredith remembers. “She and her husband adopted a cat and chose to name it after me. The patient has since passed on, but the cat lives on. It sits on her husband’s CPAP machine and turns it off for him every morning. The fact that a part of my bond with her lives on makes me exceedingly happy.” Communication has always been at the heart of such relationships, and never has it been more important in remaining connected with patients than in 2020. “The recent pandemic has created new challenges for everyone, including the health-care system,” Meredith says. “For me, it has reinforced the critical importance of communication in health care. The pandemic has impacted the way that we care for patients directly, the way that we keep their families involved and updated while their loved one is hospitalized, and the way that we communicate with community leaders and with other physicians.”
 Why did Ray Newman become a doctor? Let him count the ways: “I am reminded when I see a medical student do something the way I taught them,” he says. “I am reminded when I hear about the accomplishment of a physician I helped teach as a resident. I am reminded when I am able to reassure a parent. I am reminded when one of my patients feels better.” All of those, he says, “fill me with a sense of gratitude and fulfillment I hope everyone is lucky enough to experience in their profession.” That’s the energy this native of Aberdeen, S.D., brings to Kansas City’s medical community, with a world view informed by an All-American upbringing. He’s the son of educators who valued it highly, raised in a nuclear family that ate dinner together every night, and went to church together on Sundays. And the older he got, “the more I realized how lucky I had been as a younger person,” Newman says. “I had role models, encouragement, support, and safety while I was growing up. I think that informs my patient care today. I try to provide support to those patients who may not have a strong support system. I try to encourage and those patients who may not have a cheerleader in their life. I try to make sure the kids I see in are in safe and nurturing environments. And lastly, I try to be honest with patients and their parents when providing education or counsel.” A would-be music major in college, the tenor sax yielded to math, chemistry, and biology, classes he found both challenging and fascinating. Medicine offered something that was missing—a human connection, especially with young patients. “As I started my clinical rotations, I found that I always gravitated to the care of children. In family medicine, I wanted to see the kids. In the ER, I wanted to see the kids. On OB/Gyn, I wanted to stay with the baby after he/she was born,” Newman says. “I enjoyed the energy of the pediatric patients and I enjoyed their parents. What could be better that making a child feel better … or easing the worry of a parent? I found that I loved the people who worked in the field of pediatrics…it was like I had found my people.” Now, on the faculty at Kansas City University, and serving as chief medical officer at KCU’s Score 1 for Health preventive health program, he’s again in touch with the educator’s mindset he saw in his parents. “I want these young physicians-to-be to know what an AMAZING adventure awaits them,” he says. “I want them to know that all the hard work of medical school and residency is absolutely worth it! I have learned so many things from people who taught me and I want to share that with young physicians.”
Why did Ray Newman become a doctor? Let him count the ways: “I am reminded when I see a medical student do something the way I taught them,” he says. “I am reminded when I hear about the accomplishment of a physician I helped teach as a resident. I am reminded when I am able to reassure a parent. I am reminded when one of my patients feels better.” All of those, he says, “fill me with a sense of gratitude and fulfillment I hope everyone is lucky enough to experience in their profession.” That’s the energy this native of Aberdeen, S.D., brings to Kansas City’s medical community, with a world view informed by an All-American upbringing. He’s the son of educators who valued it highly, raised in a nuclear family that ate dinner together every night, and went to church together on Sundays. And the older he got, “the more I realized how lucky I had been as a younger person,” Newman says. “I had role models, encouragement, support, and safety while I was growing up. I think that informs my patient care today. I try to provide support to those patients who may not have a strong support system. I try to encourage and those patients who may not have a cheerleader in their life. I try to make sure the kids I see in are in safe and nurturing environments. And lastly, I try to be honest with patients and their parents when providing education or counsel.” A would-be music major in college, the tenor sax yielded to math, chemistry, and biology, classes he found both challenging and fascinating. Medicine offered something that was missing—a human connection, especially with young patients. “As I started my clinical rotations, I found that I always gravitated to the care of children. In family medicine, I wanted to see the kids. In the ER, I wanted to see the kids. On OB/Gyn, I wanted to stay with the baby after he/she was born,” Newman says. “I enjoyed the energy of the pediatric patients and I enjoyed their parents. What could be better that making a child feel better … or easing the worry of a parent? I found that I loved the people who worked in the field of pediatrics…it was like I had found my people.” Now, on the faculty at Kansas City University, and serving as chief medical officer at KCU’s Score 1 for Health preventive health program, he’s again in touch with the educator’s mindset he saw in his parents. “I want these young physicians-to-be to know what an AMAZING adventure awaits them,” he says. “I want them to know that all the hard work of medical school and residency is absolutely worth it! I have learned so many things from people who taught me and I want to share that with young physicians.”
 They don’t happen every day, but when your relationship with a patient is at the core of what you do, humbling moments can arrive out of the blue. They’ll show up in a hand-written note delivered to your desk. “When I read those thank-you notes from a patient, a spouse or a widow, I am reminded and humbled by the meaningful impact I have on patient care,” says cardiologist David Skolnick. He’s a vital cog in Saint Luke’s prominent cardiology program. He leads the health system’s echocardiography laboratory, and his interest in heart-valve disease led to his role in establishing the first valve center of excellence in the Kansas City area—a huge development for heart patients in this region. “Life-saving and innovative transcatheter valve technology has revolutionized our approach to patient care,” says Skolnick. “The majority of our patients no longer need open-heart surgery to address valve pathology. In conjunction with my interventional cardiology and surgical colleagues, our team at Saint Luke’s continues to be on the forefront of research and clinical trials for catheter-based valve intervention.” His road to cardiology came during the grueling decade of medical school and residency, when, he says, “I was fortunate to interact with some extraordinarily bright and inspiring mentors. Intrigued by the physics of cardiac function—the mechanics of how the heart works—he says “cardiology remains a rapidly evolving field, with many new therapeutic options to improve quality of life and reduce mortality.” Skolnick’s first exposure to medicine came early: His father is an emeritus professor of radiology at the University of Pittsburgh who directed the ultrasound department as that function was gaining prominence in the university hospital’s renowned kidney and liver transplant program. “My parents and their parents placed a high value on learning,” Skolnick says. “Education never ends, and I have become a life-long learner. I believe that this commitment to learning, and to teaching, serves my patients well.” He started college with an eye on chemistry, but veered into medicine, then did a year in a research lab at Ecole Polytechnique Federale de Lausanne, in Switzerland, (If you’d prefer to discuss your cardiology needs with a doctor in French, Skolnick is your man.) He met his bride-to-be while training at Washington University in St. Louis, and through some of her law-school friends from here, discovered Kansas City. Here, he has found not only professional fulfillment and challenge, but “rich offerings of great sports, music and the arts.”
They don’t happen every day, but when your relationship with a patient is at the core of what you do, humbling moments can arrive out of the blue. They’ll show up in a hand-written note delivered to your desk. “When I read those thank-you notes from a patient, a spouse or a widow, I am reminded and humbled by the meaningful impact I have on patient care,” says cardiologist David Skolnick. He’s a vital cog in Saint Luke’s prominent cardiology program. He leads the health system’s echocardiography laboratory, and his interest in heart-valve disease led to his role in establishing the first valve center of excellence in the Kansas City area—a huge development for heart patients in this region. “Life-saving and innovative transcatheter valve technology has revolutionized our approach to patient care,” says Skolnick. “The majority of our patients no longer need open-heart surgery to address valve pathology. In conjunction with my interventional cardiology and surgical colleagues, our team at Saint Luke’s continues to be on the forefront of research and clinical trials for catheter-based valve intervention.” His road to cardiology came during the grueling decade of medical school and residency, when, he says, “I was fortunate to interact with some extraordinarily bright and inspiring mentors. Intrigued by the physics of cardiac function—the mechanics of how the heart works—he says “cardiology remains a rapidly evolving field, with many new therapeutic options to improve quality of life and reduce mortality.” Skolnick’s first exposure to medicine came early: His father is an emeritus professor of radiology at the University of Pittsburgh who directed the ultrasound department as that function was gaining prominence in the university hospital’s renowned kidney and liver transplant program. “My parents and their parents placed a high value on learning,” Skolnick says. “Education never ends, and I have become a life-long learner. I believe that this commitment to learning, and to teaching, serves my patients well.” He started college with an eye on chemistry, but veered into medicine, then did a year in a research lab at Ecole Polytechnique Federale de Lausanne, in Switzerland, (If you’d prefer to discuss your cardiology needs with a doctor in French, Skolnick is your man.) He met his bride-to-be while training at Washington University in St. Louis, and through some of her law-school friends from here, discovered Kansas City. Here, he has found not only professional fulfillment and challenge, but “rich offerings of great sports, music and the arts.”
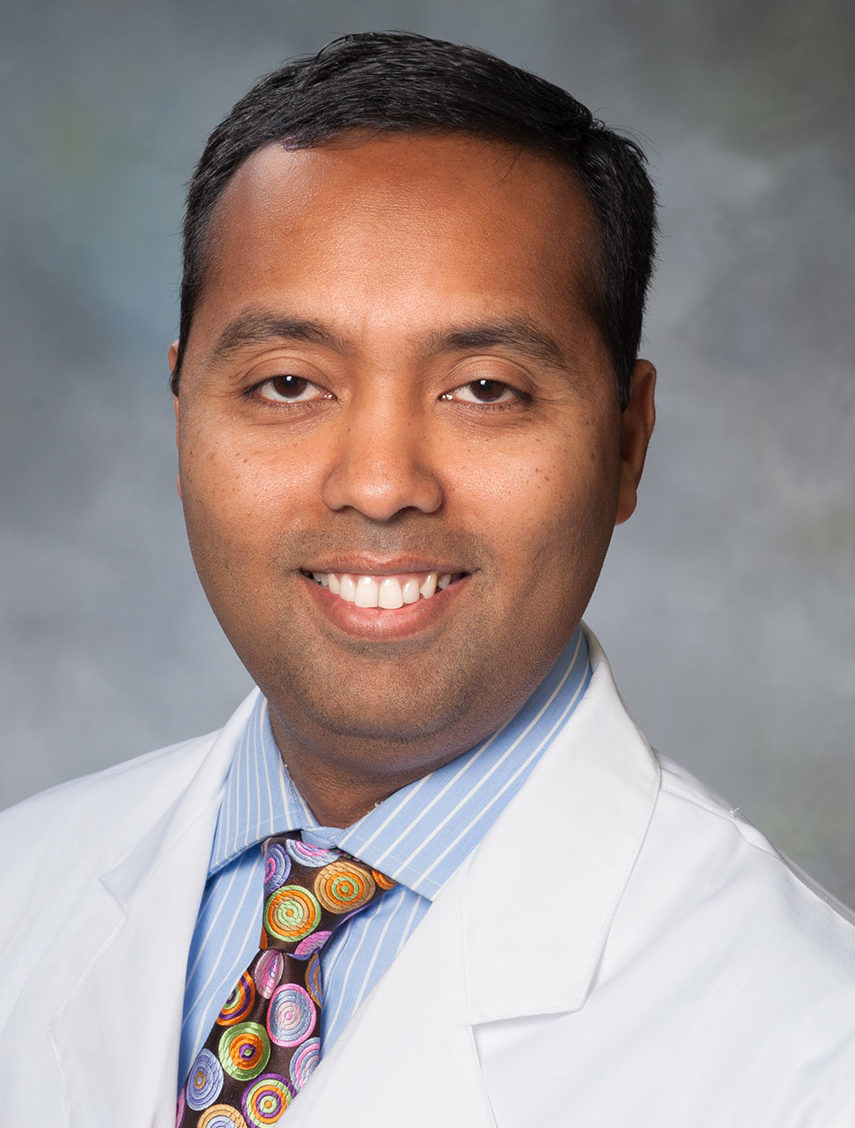 To become the kind of oncologist he hoped he would be, Janakiraman Subramanian made a commitment to himself: He wouldn’t be the kind to tell a patient there was nothing that could be done. He’d seen that once while still in his medical training in India, as another doctor told a man suffering from late-stage abdominal cancer to go home and spend time with his family. “Your end is here,” he said. “That was incredibly sad,” Subramanian recalls. “It feels so helpless when you say there is nothing more we can do. In some ways, it is our failure as physicians. I don’t want to an have interaction like that.” That he’s living out his commitment, and doing it in Kansas City, is testament to the innovation Saint Luke’s is bringing to cancer research. Subramanian is co-director for the system’s Center for Precision Oncology, which melds clinical oncology, tumor genomics, and computational biology in a quest for personalized cancer treatments. “We think of cancer as a disease, and that is true, but even people who know more, and know there are different types still think in terms of similar treatments: For breast cancer, there is a particular type of treatment. For lung cancer, a particular type.” But once you get past those boilerplate treatments, and they don’t work, where are you? “Then there are very limited options,” Subramanian says. “Precision oncology is trying to find, apart from those standard treatments, additional options. These patients are running out of options as the disease progresses.” His work aims to find, at a genetic level, individualized treatments that can buy precious time. It’s very personalized, very directed toward that patient,” he says. Prodded by his father, a physics professor with an ironclad commitment to education, Subramanian ended up in medicine and had his first exposure to the U.S. with a stint in Wichita. There, he was deeply impressed by the reception he received, and by the willingness of others to help him succeed. “They went beyond common courtesy,” he says. He later set up shop at Washington University in St. Louis before Saint Luke’s came calling. “Where I am right now, it’s a good place to be, for several reasons,” he says. “One, I get to practice my field, thoracic cancer, at an institution that is incredibly supportive with programs I want on the clinical side and research I want to do.” Another reason is the type of people here, tying back to the Midwestern values. “I did a brief stint in Knoxville, Tennessee, but came right back to the Midwest. I don’t know if it was fate or fortune.”
To become the kind of oncologist he hoped he would be, Janakiraman Subramanian made a commitment to himself: He wouldn’t be the kind to tell a patient there was nothing that could be done. He’d seen that once while still in his medical training in India, as another doctor told a man suffering from late-stage abdominal cancer to go home and spend time with his family. “Your end is here,” he said. “That was incredibly sad,” Subramanian recalls. “It feels so helpless when you say there is nothing more we can do. In some ways, it is our failure as physicians. I don’t want to an have interaction like that.” That he’s living out his commitment, and doing it in Kansas City, is testament to the innovation Saint Luke’s is bringing to cancer research. Subramanian is co-director for the system’s Center for Precision Oncology, which melds clinical oncology, tumor genomics, and computational biology in a quest for personalized cancer treatments. “We think of cancer as a disease, and that is true, but even people who know more, and know there are different types still think in terms of similar treatments: For breast cancer, there is a particular type of treatment. For lung cancer, a particular type.” But once you get past those boilerplate treatments, and they don’t work, where are you? “Then there are very limited options,” Subramanian says. “Precision oncology is trying to find, apart from those standard treatments, additional options. These patients are running out of options as the disease progresses.” His work aims to find, at a genetic level, individualized treatments that can buy precious time. It’s very personalized, very directed toward that patient,” he says. Prodded by his father, a physics professor with an ironclad commitment to education, Subramanian ended up in medicine and had his first exposure to the U.S. with a stint in Wichita. There, he was deeply impressed by the reception he received, and by the willingness of others to help him succeed. “They went beyond common courtesy,” he says. He later set up shop at Washington University in St. Louis before Saint Luke’s came calling. “Where I am right now, it’s a good place to be, for several reasons,” he says. “One, I get to practice my field, thoracic cancer, at an institution that is incredibly supportive with programs I want on the clinical side and research I want to do.” Another reason is the type of people here, tying back to the Midwestern values. “I did a brief stint in Knoxville, Tennessee, but came right back to the Midwest. I don’t know if it was fate or fortune.”
 Two things about 2020 have confirmed Steve Stites’ decision to become a doctor. One, of course, is the small matter of a global pandemic. It has made the chief medical officer at the University of Kansas Hospital an in-house media star, thanks to the daily briefings he leads most days from the anchor desk on the hospital’s video set. The other development—a social-justice movement that has rocked the nation—connects with a deeply personal part of his professional past. “I think about it a lot,” he says. “When I was a resident back east, a young man in
Two things about 2020 have confirmed Steve Stites’ decision to become a doctor. One, of course, is the small matter of a global pandemic. It has made the chief medical officer at the University of Kansas Hospital an in-house media star, thanks to the daily briefings he leads most days from the anchor desk on the hospital’s video set. The other development—a social-justice movement that has rocked the nation—connects with a deeply personal part of his professional past. “I think about it a lot,” he says. “When I was a resident back east, a young man in
ICU—I’ll always remember this—came in with fluid around his heart. He was pretty sick.” But some on the medical staff had prejudged the patient, who was African-American, writing his condition off as a likely drug overdose. He didn’t get the immediate treatment he needed. It turned out, Stites said, that patient was suffering from a reaction to recent dental work, leading to a serious heart infection. “I will never forget the anguish of the family and how people had misjudged him from the start,” Stites says. “I knew this was going badly and that we couldn’t save him. People judged him and didn’t do the right thing, and by the time he was in the ICU, the writing was on the wall.” Stites repeats that story often, he says, “because there are so many teachable moments in that. It carries home about how you have to treat everybody.” That same concern over the welfare of patients is now a concern for an entire metro area’s population; Stites has been a vocal and consistent advocate for the kinds of personal responsibility and individual actions needed to rein in a global pandemic. Anyone who knows him has probably heard is cautionary mantra of the past eight months: Wash your hands frequently, stay home if you’re sick, wear a mask, stay six feet apart, don’t touch your face. Back in the late winter, that message was driven in part by fears that the medical system would be overwhelmed with coronavirus caseloads, threatening the very care-givers attempting human damage control. Now, he’s looking out for everyone. “I tell everybody now my job is to be honest, truthful and calm,” Stites says. “So much in the media is what I call flapjacking: People who flap their arms and jack with the truth. It happens on both sides of the aisle. The other problem with COVID is that so much time is spent talking about the stats by people who don’t remember that at any one time, 1 percent of the people out there may have it, and it’s our job to treat them—but our job is also to protect the 99 percent who don’t.”
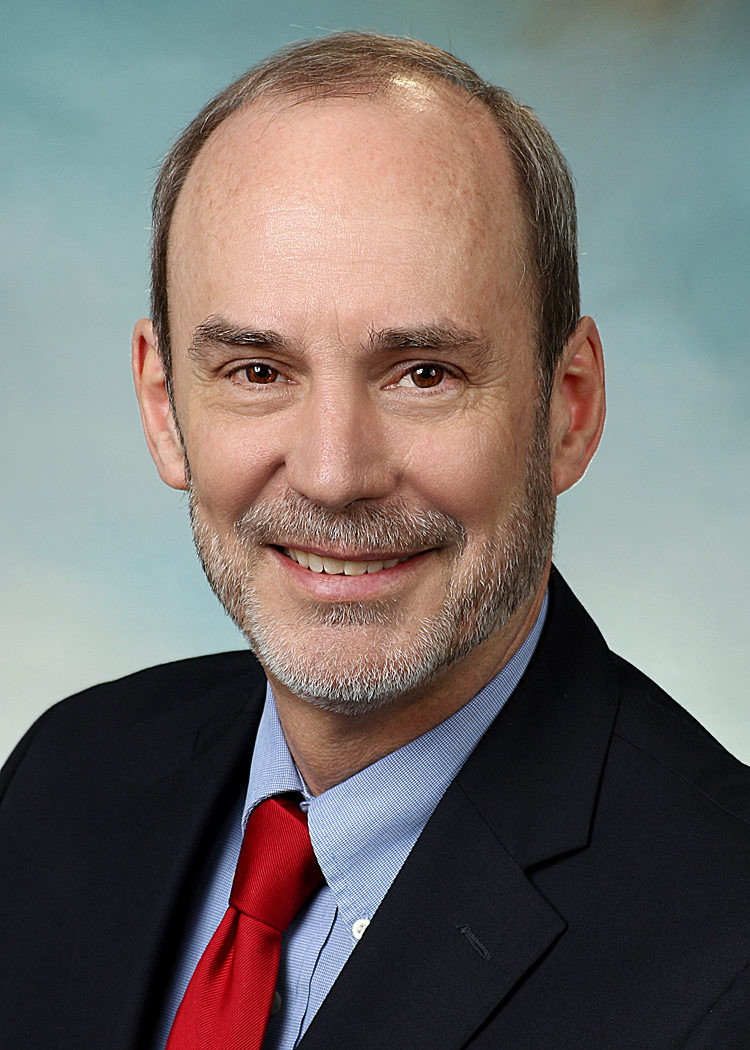 It was just another day at the office for Jim Wetzel, but the particular moment sticks with him. An internal medicine specialist by practice, he ordered up a CT scan for a patient, as he’d done for so many others for years. “Doctor,” the woman asked, “you have probably ordered hundreds of these over the years, haven’t you?” Affirmative, he replied. “Her next comment was, “well this is my first CT,” Wetzel recalls. And there-in was his lesson: “I learned that patients want to understand, and it was my job to educate them to the best of my ability.” He’s an Iowa native who grew up on a farm, and his parents instilled in him traditional values of love for the land, a sense of gratitude for opportunity, and a drive to excel. A ken for journalism gave way to his true love, science, and “as I contemplated career opportunities, I knew I liked science and I like people,” Wetzel says. “I did not think I was suited for research or for teaching. Medicine seemed like the ideal for me.” Internal medicine was appealing, he said, because it “is like putting together pieces of a puzzle. How do symptoms and test results help reach a diagnosis? Patients want to know what is wrong, even when the news is not positive.” Medicine has changed a lot over his career, but perhaps more in the past year than any before. “COVID,” he says, “has forced us to consider how we can take care of our patients when they fear being seen in person. Telehealth, phone visits, innovative ways to avoid waiting in close quarters and coordinating visits to minimize risks are all necessary.” From a population standpoint, he says, offering what appears to be high-touch with physical distancing and electronics visits and monitoring offers the promise of better patient care. “Everyone has done their best with COVID, and we have all learned a lot. Certainly, that will help in the event of another pandemic.” Now the hospital’s chief medical officer, he can look back over a career filled with professional satisfaction from knowing that he can change people’s lives—even when if it takes some time to get there. He witnessed that with a patient who had been a heavy smoker and frequent imbiber. “At each visit, I reminded him that his habits had consequences to health and longevity. This went on for a decade,” Wetzel says. “Then one visit when I asked him about his habits, very surprisingly, he told me he had quit smoking and drinking entirely. I asked him why he quit and he said, “Because you told me I needed to.” That was proof that perseverance, gentle nudging and follow-up will eventually yield results.”
It was just another day at the office for Jim Wetzel, but the particular moment sticks with him. An internal medicine specialist by practice, he ordered up a CT scan for a patient, as he’d done for so many others for years. “Doctor,” the woman asked, “you have probably ordered hundreds of these over the years, haven’t you?” Affirmative, he replied. “Her next comment was, “well this is my first CT,” Wetzel recalls. And there-in was his lesson: “I learned that patients want to understand, and it was my job to educate them to the best of my ability.” He’s an Iowa native who grew up on a farm, and his parents instilled in him traditional values of love for the land, a sense of gratitude for opportunity, and a drive to excel. A ken for journalism gave way to his true love, science, and “as I contemplated career opportunities, I knew I liked science and I like people,” Wetzel says. “I did not think I was suited for research or for teaching. Medicine seemed like the ideal for me.” Internal medicine was appealing, he said, because it “is like putting together pieces of a puzzle. How do symptoms and test results help reach a diagnosis? Patients want to know what is wrong, even when the news is not positive.” Medicine has changed a lot over his career, but perhaps more in the past year than any before. “COVID,” he says, “has forced us to consider how we can take care of our patients when they fear being seen in person. Telehealth, phone visits, innovative ways to avoid waiting in close quarters and coordinating visits to minimize risks are all necessary.” From a population standpoint, he says, offering what appears to be high-touch with physical distancing and electronics visits and monitoring offers the promise of better patient care. “Everyone has done their best with COVID, and we have all learned a lot. Certainly, that will help in the event of another pandemic.” Now the hospital’s chief medical officer, he can look back over a career filled with professional satisfaction from knowing that he can change people’s lives—even when if it takes some time to get there. He witnessed that with a patient who had been a heavy smoker and frequent imbiber. “At each visit, I reminded him that his habits had consequences to health and longevity. This went on for a decade,” Wetzel says. “Then one visit when I asked him about his habits, very surprisingly, he told me he had quit smoking and drinking entirely. I asked him why he quit and he said, “Because you told me I needed to.” That was proof that perseverance, gentle nudging and follow-up will eventually yield results.”
